Advancements in Treatment for Hearing Loss with Hearing Aids
Hearing loss is a prominent condition, the risk of which may be affected by many factors. These include advancing age, structural defects, infection, certain neurological and/or genetic conditions and trauma to the ear or skull1,2. Hearing loss may be experienced in one ear or both3. There is a long-established history of devices intended to address this problem. This ranges from stereotypical images of ‘ear trumpets’ to sophisticated devices that may be implanted into the body to address hearing issues3. They are known as hearing-assistive devices or more commonly as hearing aids.
 Cochlear Implant Surgery
Cochlear Implant Surgery
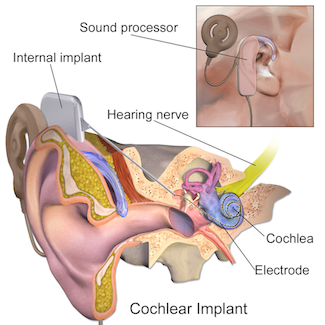
Cochlear implants may address the issues of hearing loss in one ear, and restore at least some of the links with the internal and external ear that are often damaged by many forms of hearing loss4. These implants, as the name suggests, consist of an electrode placed in or near the cochlea of the inner ear. This is connected to a receiver or stimulator (which is usually also implanted), an external transmitter and a battery pack which may be worn over the ear. The electrode stimulates the auditory nerve to pick up and process sounds when activated. Some researchers regard the cochlear implant as a particularly effective solution for hearing loss associated with congenital defects, trauma and other damage such as that sustained in removing a tumor from the skull or brain4.
Contralateral routing of signal hearing aids (CROS) are devices that utilize a microphone placed in an ear affected by hearing loss, to amplify sounds. These sounds are immediately conveyed to a receiver in the less-affected ear. Bilateral CROS (BICROS) consists of microphones in both ears, connected to a single amplifier and to a receiver. This is placed in the less-affected ear, so that it benefits from both sound amplification and the input from the more-affected ear. Some forms of BICROS are also equipped with noise reduction technology, with a view to reducing background noise and improving voice recognition5. However, a recent study indicated that this development had limited effect on sentence recognition for its 21 participants (patients with asymmetric hearing loss and experience using BICROS)5.
Bone Conduction Hearing Aids
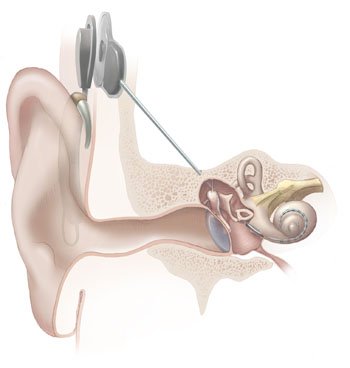 Other state-of-the-art forms of hearing aids enhance sound perception through bone conduction. These devices augment or supplant sounds conducted to the middle ear through the air, which is the predominant method of sound conduction for those with normal hearing. They may be affixed to the outside of the skull (i.e. transcutaneously), or be incorporated into this bone through the skin (percutaneously)6,7. These ‘bone-anchored’ devices are minimally obtrusive and visible, thus potentially increasing its acceptability to patients8. They are suitable for patients with hearing loss in one or both ears7. An emerging variation on this technology is a percutaneous bone-anchored device in combination with an additional circular magnet containing a digital auditory processor, which is inserted under the skin7.
Other state-of-the-art forms of hearing aids enhance sound perception through bone conduction. These devices augment or supplant sounds conducted to the middle ear through the air, which is the predominant method of sound conduction for those with normal hearing. They may be affixed to the outside of the skull (i.e. transcutaneously), or be incorporated into this bone through the skin (percutaneously)6,7. These ‘bone-anchored’ devices are minimally obtrusive and visible, thus potentially increasing its acceptability to patients8. They are suitable for patients with hearing loss in one or both ears7. An emerging variation on this technology is a percutaneous bone-anchored device in combination with an additional circular magnet containing a digital auditory processor, which is inserted under the skin7.
Other forms of implanted devices are used to replace or augment damaged and/or dysfunctional parts of the internal ear2. Some or all components of this hearing aid type (including the power source) are placed surgically within the middle ear2. Eligible candidates for this option are typically adult patients with moderate to severe hearing loss (which may be the result of congenital defect or infection) that does not respond to the less invasive options mentioned above2. Examples of implantable hearing aid products available and approved by regulatory bodies include Esteem®, Carina®, Vibrant Soundbridge® and Maxum® devices2.
Without a doubt, these advancements in hearing assistance can improve patient life quality through an increase in sound perception, and may also maintain or improve the social and functional status of patients affected by hearing loss9,10.
A modified version of this article was showcased on the doctor powered blog at md.com. To read the other source go here.
References:
- Lin FR, Thorpe R, Gordon-Salant S, Ferrucci L. Hearing loss prevalence and risk factors among older adults in the United States. J Gerontol A Biol Sci Med Sci. 2011;66(5):582-590.
- Bittencourt AG, Burke PR, Jardim IdS, et al. Implantable and Semi-Implantable Hearing Aids: A Review of History, Indications, and Surgery. International Archives of Otorhinolaryngology. 2014;18(3):303-310.
- Kitterick PT, Lucas L, Smith SN. Improving Health-Related Quality of Life in Single-Sided Deafness: A Systematic Review and Meta-Analysis. Audiol Neurootol. 2015;20 Suppl 1:79-86.
- Wilson BS, Dorman MF. Cochlear implants: a remarkable past and a brilliant future. Hearing research. 2008;242(0):3-21.
- Oeding K, Valente M. Sentence recognition in noise and perceived benefit of noise reduction on the receiver and transmitter sides of a BICROS hearing aid. J Am Acad Audiol. 2013;24(10):980-991.
- Leterme G, Bernardeschi D, Bensemman A, et al. Contralateral Routing of Signal Hearing Aid versus Transcutaneous Bone Conduction in Single-Sided Deafness. Audiol Neurootol. 2015;20(4):251-260.
- Marsella P, Scorpecci A, Dalmasso G, Pacifico C. First experience in Italy with a new transcutaneous bone conduction implant. Acta Otorhinolaryngol Ital. 2015;35(1):29-33.
- Reinfeldt S, Hakansson B, Taghavi H, Eeg-Olofsson M. New developments in bone-conduction hearing implants: a review. Med Devices (Auckl). 2015;8:79-93.
- Douglas SA, Yeung P, Daudia A, Gatehouse S, O’Donoghue GM. Spatial hearing disability after acoustic neuroma removal. Laryngoscope. 2007;117(9):1648-1651.
- Hornsby BW. The effects of hearing aid use on listening effort and mental fatigue associated with sustained speech processing demands. Ear Hear. 2013;34(5):523-534.